|
HIV - AIDS
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
HOME | BIOLOGY | FILMS | GEOGRAPHY | HISTORY | INDEX | MUSIC | SOLAR BOATS | SPORT | SPONSORS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Human immunodeficiency virus or HIV is a retrovirus that causes Acquired Immunodeficiency Syndrome (AIDS), a condition in which the immune system begins to fail, leading to life-threatening opportunistic infections. Previous names for the virus include Human T-Lymphotropic Virus-III (HTLV-III) and lymphadenopathy-associated virus (LAV).
Infection with HIV occurs by the transfer of blood, semen, vaginal fluid, Cowper's fluid or breast milk. Within these body fluids HIV is present as both free virus particles and virus within infected immune cells. The three major routes of transmission are unprotected sexual intercourse, contaminated needles and transmission from an infected mother to her baby at birth or through breast milk. Screening of blood products for HIV in the developed world has largely eliminated transmission through blood transfusions or infected blood products in these countries.
HIV infection in humans is now pandemic. As of January 2006, the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the World Health Organization (WHO) estimate that AIDS has killed more than 25 million people since it was first recognized on December 1, 1981, making it one of the most destructive pandemics in recorded history. In 2005 alone, AIDS claimed an estimated 2.4-3.3 million lives, of which more than 570,000 were children. A third of these deaths are occurring in sub-Saharan Africa, retarding economic growth and increasing poverty. According to current estimates, HIV is set to infect 90 million people in Africa, resulting in a minimum estimate of 18 million orphans. Antiretroviral treatment reduces both the mortality and the morbidity of HIV infection, but routine access to antiretroviral medication is not available in all countries.
HIV primarily infects vital cells in the human immune system such as helper T cells (specifically CD4+ T cells), macrophages and dendritic cells. HIV infection leads to low levels of CD4+ T cells through three main mechanisms: firstly, direct viral killing of infected cells; secondly, increased rates of apoptosis in infected cells; and thirdly, killing of infected CD4+ T cells by CD8 cytotoxic lymphocytes that recognize infected cells. When CD4+ T cell numbers decline below a critical level, cell-mediated immunity is lost, and the body becomes progressively more susceptible to opportunistic infections. If untreated, eventually most HIV-infected individuals develop AIDS and die; however about one in ten remain healthy for many years, with no noticeable symptoms. Treatment with anti-retrovirals, where available, increases the life expectancy of people infected with HIV. It is hoped that current and future treatments may allow HIV-infected individuals to achieve a life expectancy approaching that of the general public (see Treatment).
Origin and discovery
The AIDS epidemic was discovered June 5, 1981, when the U.S. Centers for Disease Control and Prevention reported a cluster of Pneumocystis carinii pneumonia (now classified as Pneumocystis jiroveci pneumonia) in five homosexual men in Los Angeles. The disease was originally dubbed GRID, or Gay-Related Immune Deficiency, but health authorities soon realized that nearly half of the people identified with the syndrome were not homosexual men. In 1982, the CDC introduced the term AIDS to describe the newly recognized syndrome, though it was still casually referred to as GRID.
In 1983, scientists led by Luc Montagnier at the Pasteur Institute in France first discovered the virus that causes AIDS. They called it lymphadenopathy-associated virus (LAV). A year later a team led by Robert Gallo of the United States confirmed the discovery of the virus, but they renamed it human T lymphotropic virus type III (HTLV-III). The dual discovery led to considerable scientific disagreement, and it was not until President Mitterrand of France and President Reagan of the USA met that the major issues were resolved. In 1986, both the French and the US names for the virus itself were dropped in favour of the new term, human immunodeficiency virus (HIV).
HIV was classified as a member of the genus lentivirus, part of the family of retroviridae. Lentiviruses have many common morphologies and biological properties. Many species are infected by lentiviruses, which are characteristically responsible for long-duration illnesses with a long incubation period. Lentiviruses are transmitted as single-stranded, positive-sense, enveloped RNA viruses. Upon entry of the target cell, the viral RNA genome is converted to double-stranded DNA by a virally encoded reverse transcriptase that is present in the virus particle. This viral DNA is then integrated into the cellular DNA by a virally encoded integrase so that the genome can be transcribed. Once the virus has infected the cell, two pathways are possible: either the virus becomes latent and the infected cell continues to function, or the virus becomes active and replicates, and a large number of virus particles are liberated that can then infect other cells.
Two species of HIV infect humans: HIV-1 and HIV-2. HIV-1 is thought to have originated in southern Cameroon after jumping from wild chimpanzees (Pan troglodytes troglodytes) to humans during the twentieth century. HIV-2 may have originated from the Sooty Mangabey (Cercocebus atys), an Old World monkey of Guinea-Bissau, Gabon, and Cameroon. HIV-1 is the most virulent. It is easily transmitted and is the cause of the majority of HIV infections globally. HIV-2 is less transmittable and is largely confined to West Africa. HIV-1 is the virus that was initially discovered and termed LAV.
Three of the earliest known instances of HIV-1 infection are as follows:
Although a variety of theories exist explaining the transfer of HIV to humans, no single hypothesis is widely accepted, and the topic remains controversial. Freelance journalist Tom Curtis discussed one controversial possibility for the origin of HIV/AIDS in a 1992 Rolling Stone magazine article. He put forward what is now known as the OPV AIDS hypothesis, which suggests that AIDS was inadvertently caused in the late 1950s in the Belgian Congo by Hilary Koprowski's research into a polio vaccine. Although subsequently retracted due to libel issues surrounding its claims, the Rolling Stone article motivated another freelance journalist, Edward Hooper, to probe more deeply into this subject. Hooper's research resulted in his publishing a 1999 book, The River, in which he alleged that an experimental oral polio vaccine prepared using chimpanzee kidney tissue was the route through which simian immunodeficiency virus (SIV) crossed into humans to become HIV, thus starting the human AIDS pandemic. This theory is contradicted by an analysis of genetic mutation in primate lentivirus strains that indicates with 95% certainty that the origin of the HIV-1 strain dates to about 1930.
Since the beginning of the pandemic, three main transmission routes for HIV have been identified
Transmission
HIV-2 is transmitted much less frequently by the MTCT and sexual route than HIV-1.
HIV has been found at low concentrations in the saliva, tears and urine of infected individuals, but the risk of transmission by these secretions is negligible. The use of physical barriers such as the latex condom is widely advocated to reduce the sexual transmission of HIV. Spermicide when used alone or with vaginal contraceptives like a diaphragm actually increases the male to female transmission rate due to inflammation of the vagina, and should not be considered a barrier to infection. Current research is clarifying the relationship between male circumcision and HIV in differing social and cultural contexts. Even though male circumcision may lead to a reduction of infection risk in heterosexual men by up to 60%, UNAIDS believes that it is premature to recommend male circumcision as part of HIV prevention programs. South African medical experts are concerned that the repeated use of unsterilized blades in the ritual circumcision of adolescent boys may be spreading HIV.
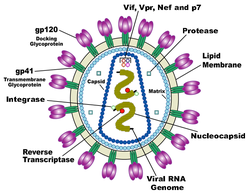
Diagram of HIV
Structure and genome
HIV is different in structure from other retroviruses. It is about 120 nm in diameter (120 billionths of a meter; around 60 times smaller than a red blood cell) and roughly spherical.
It is composed of two copies of positive single-stranded RNA that codes for the virus's nine genes enclosed by a conical capsid composed of 2,000 copies of the viral protein, p24. The single-stranded RNA is tightly bound to nucleocapsid proteins, p7 and enzymes needed for the development of the virion such as reverse transcriptase, proteases and integrase. A matrix composed of the viral protein p17 surrounds the capsid ensuring the integrity of the virion particle. This is, in turn, surrounded by the viral envelope which is composed of two layers of fatty molecules called phospholipids taken from the membrane of a human cell when a newly formed virus particle buds from the cell. Embedded in the viral envelope are proteins from the host cell and about 70 copies of a complex HIV protein that protrudes through the surface of the virus particle. This protein, known as Env, consists of a cap made of three molecules called glycoprotein (gp) 120, and a stem consisting of three gp41 molecules that anchor the structure into the viral envelope. This glycoprotein complex enables the virus to attach to and fuse with target cells to initiate the infectious cycle. Both these surface proteins, especially gp120, have been considered as targets of future treatments or vaccines against HIV.
Of the nine genes that are encoded within the RNA genome, three of these genes, gag, pol, and env, contain information needed to make the structural proteins for new virus particles. env, for example, codes for a protein called gp160 that is broken down by a viral enzyme to form gp120 and gp41. The six remaining genes, tat, rev, nef, vif, vpr, and vpu (or vpx in the case of HIV-2), are regulatory genes for proteins that control the ability of HIV to infect cells, produce new copies of virus (replicate), or cause disease. The protein encoded by nef, for instance, appears necessary for the virus to replicate efficiently, and the vpu-encoded protein influences the release of new virus particles from infected cells. The ends of each strand of HIV RNA contain an RNA sequence called the long terminal repeat (LTR). Regions in the LTR act as switches to control production of new viruses and can be triggered by proteins from either HIV or the host cell.
Tropism
The term viral tropism refers to which cell types HIV infects. HIV can infect a variety of immune cells such as CD4+ T cells, macrophages, and microglial cells. HIV-1 entry to macrophages and CD4+ T cells is mediated through interaction of the virion envelope glycoproteins (gp120) with the CD4 molecule on the target cells and also with chemokine coreceptors.
Macrophage (M-tropic) strains of HIV-1, or non-syncitia-inducing strains (NSI) use the β-chemokine receptor CCR5 for entry and are thus able to replicate in macrophages and CD4+ T cells. This CCR5 coreceptor is used by almost all primary HIV-1 isolates regardless of viral genetic subtype. Indeed, macrophages play a key role in several critical aspects of HIV infection. They appear to be the first cells infected by HIV and perhaps the source of HIV production when CD4+ cells become depleted in the patient. Macrophages and microglial cells are the cells infected by HIV in the central nervous system. In tonsils and adenoids of HIV-infected patients, macrophages fuse into multinucleated giant cells that produce huge amounts of virus.
T-tropic isolates, or syncitia-inducing (SI) strains replicate in primary CD4+ T cells as well as in macrophages and use the α-chemokine receptor, CXCR4, for entry. The α-chemokine, SDF-1, a ligand for CXCR4, suppresses replication of T-tropic HIV-1 isolates. It does this by down-regulating the expression of CXCR4 on the surface of these cells. HIV that use only the CCR5 receptor are termed R5, those that only use CXCR4 are termed X4, and those that use both, X4R5. However, the use of coreceptor alone does not explain viral tropism, as not all R5 viruses are able to use CCR5 on macrophages for a productive infection and HIV can also infect a subtype of myeloid dendritic cells, which probably constitute a reservoir that maintains infection when CD4+ T cell numbers have declined to extremely low levels.
Some people are resistant to certain strains of HIV. One example of how this occurs is people with the CCR5-Δ32 mutation; these people are resistant to infection with R5 virus as the mutation stops HIV from binding to this coreceptor, reducing its ability to infect target cells.
Heterosexual intercourse is the major mode of HIV transmission. Both X4 and R5 HIV are present in the seminal fluid which is passed from partner to partner. The virions can then infect numerous cellular targets and disseminate into the whole organism. However, a selection process leads to a predominant transmission of the R5 virus through this pathway. How this selective process works is still under investigation, but one model is that spermatozoa may selectively carry R5 HIV as they possess both CCR3 and CCR5 but not CXCR4 on their surface and that genital epithelial cells preferentially sequester X4 virus. In patients infected with subtype B HIV-1, there is often a co-receptor switch in late-stage disease and T-tropic variants appear that can infect a variety of T cells through CXCR4. These variants then replicate more aggressively with heightened virulence that causes rapid T cell depletion, immune system collapse, and opportunistic infections that mark the advent of AIDS. Thus, during the course of infection, viral adaptation to the use of CXCR4 instead of CCR5 may be a key step in the progression to AIDS. A number of studies with subtype B-infected individuals have determined that between 40 and 50% of AIDS patients can harbour viruses of the SI, and presumably the X4, phenotype.
Replication cycle
Entry to the cell
HIV enters macrophages and CD4+ T cells by the adsorption of glycoproteins on its surface to receptors on the target cell followed by fusion of the viral envelope with the cell membrane and the release of the HIV capsid into the cell.
The interactions of the trimeric envelope complex (gp160 spike, discussed above) and both CD4 and a chemokine receptor (generally either CCR5 or CXCR4 but others are known to interact) on the cell surface. The gp160 spike contains binding domains for both CD4 and chemokine receptors. The first step in fusion involves the high-affinity attachment of the CD4 binding domains of gp120 to CD4. Once gp120 is bound with the CD4 protein, the envelope complex undergoes a structural change, exposing the chemokine binding domains of gp120 and allowing them to interact with the target chemokine receptor. This allows for a more stable two-pronged attachment, which allows the N-terminal fusion peptide gp41 to penetrate the cell membrane. Repeat sequences in gp41, HR1 and HR2 then interact, causing the collapse of the extracellular portion of gp41 into a hairpin. This loop structure brings the virus and cell membranes close together, allowing fusion of the membranes and subsequent entry of the viral capsid.
Once HIV has bound to the target cell, the HIV RNA and various enzymes, including reverse transcriptase, integrase and protease, are injected into the cell.
HIV can infect dendritic cells (DCs) by this CD4-CCR5 route, but another route using mannose-specific C-type lectin receptors such as DC-SIGN can also be used. DCs are one of the first cells encountered by the virus during sexual transmission. They are currently thought to play an important role by transmitting HIV to T cells once the virus has been captured in the mucosa by DCs.
Replication and transcription
Once the viral capsid enters the cell, an enzyme called reverse transcriptase liberates the single-stranded (+)RNA from the attached viral proteins and copies it into a complementary DNA of 9 kb size. This process of reverse transcription is extremely error-prone and it is during this step that mutations may occur. Such mutations may cause drug resistance. The reverse transcriptase then makes a complementary DNA strand to form a double-stranded viral DNA intermediate (vDNA). This vDNA is then transported into the cell nucleus. The integration of the viral DNA into the host cell's genome is carried out by another viral enzyme called integrase.
This integrated viral DNA may then lie dormant, in the latent stage of HIV infection. To actively produce the virus, certain cellular transcription factors need to be present, the most important of which is NF-κB (NF kappa B), which is upregulated when T cells become activated. This means that those cells most likely to be killed by HIV are in fact those currently fighting infection.
In this replication process, the integrated provirus is copied to mRNA which is then spliced into smaller pieces. These small pieces produce the regulatory proteins Tat (which encourages new virus production) and Rev. As Rev accumulates it gradually starts to inhibit mRNA splicing. At this stage, the structural proteins Gag and Env are produced from the full-length mRNA. The full-length RNA is actually the virus genome; it binds to the Gag protein and is packaged into new virus particles.
HIV-1 and HIV-2 appear to package their RNA differently; HIV-1 will bind to any appropriate RNA whereas HIV-2 will preferentially bind to the mRNA which was used to create the Gag protein itself. This may mean that HIV-1 is better able to mutate (HIV-1 infection progresses to AIDS faster than HIV-2 infection and is responsible for the majority of global infections)
Assembly and release
The final step of the viral cycle, assembly of new HIV-1 virons, begins at the plasma membrane of the host cell. The Env polyprotein (gp160) goes through the endoplasmic reticulum and is transported to the Golgi complex where it is cleaved by protease and processed into the two HIV envelope glycoproteins gp41 and gp120. These are transported to the plasma membrane of the host cell where gp41 anchors the gp120 to the membrane of the infected cell. The Gag (p55) and Gag-Pol (p160) polyproteins also associate with the inner surface of the plasma membrane along with the HIV genomic RNA as the forming virion begins to bud from the host cell. Maturation either occurs in the forming bud or in the immature virion after it buds from the host cell. During maturation, HIV proteases cleave the polyproteins into individual functional HIV proteins and enzymes. The various structural components then assemble to produce a mature HIV virion. This cleavage step can be inhibited by protease inhibitors. The mature virus is then able to infect another cell.
Genetic variability
HIV differs from many other viruses as it has very high genetic variability. This diversity is a result of its fast replication cycle, with the generation of 109 to 1010 virions every day, coupled with a high mutation rate of approximately 3 x 10-5 per nucleotide base per cycle of replication and recombinogenic properties of reverse transcriptase. This complex scenario leads to the generation of many variants of HIV in a single infected patient in the course of one day. This variability is compounded when a single cell is simultaneously infected by two or more different strains of HIV. When simultaneous infection occurs, the genome of progeny virions may be composed of RNA strands from two different strains. This hybrid virion then infects a new cell where it undergoes replication. As this happens, the reverse transcriptase, by jumping back and forth between the two different RNA templates, will generate a newly synthesized retroviral DNA sequence that is a recombinant between the two parental genomes. This recombination is most obvious when it occurs between subtypes.
The closely related simian immunodeficiency virus (SIV) exhibits a somewhat different behavior: in its natural hosts, African green monkeys and sooty mangabeys, the retrovirus is present in high levels in the blood, but evokes only a mild immune response, does not cause the development of simian AIDS, and does not undergo the extensive mutation and recombination typical of HIV. By contrast, infection of heterologous hosts (rhesus or cynomologus macaques) with SIV results in the generation of genetic diversity that is on the same order as HIV in infected humans; these heterologous hosts also develop simian AIDS. The relationship, if any, between genetic diversification, immune response, and disease progression is unknown.
Three groups of HIV-1 have been identified on the basis of differences in env: M, N, and O. Group M is the most prevalent and is subdivided into eight subtypes (or clades), based on the whole genome, which are geographically distinct. The most prevalent are subtypes B (found mainly in North America and Europe), A and D (found mainly in Africa), and C (found mainly in Africa and Asia); these subtypes form branches in the phylogenetic tree representing the lineage of the M group of HIV-1. Coinfection with distinct subtypes gives rise to circulating recombinant forms (CRFs). In 2000, the last year in which an analysis of global subtype prevalence was made, 47.2% of infections worldwide were of subtype C, 26.7% were of subtype A/CRF02_AG, 12.3% were of subtype B, 5.3% were of subtype D, 3.2% were of CRF_AE, and the remaining 5.3% were composed of other subtypes and CRFs. Most HIV-1 research is focused on subtype B; few laboratories focus on the other subtypes.
The genetic sequence of HIV-2 is only partially homologous to HIV-1 and more closely resembles that of SIV than HIV-1.
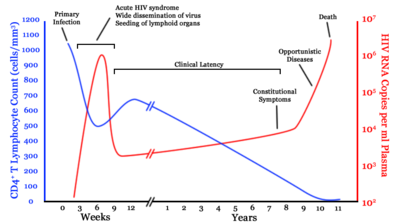
generalized graph of the relationship between HIV copies (viral load) and CD4 counts over the average course of untreated HIV infection; any particular individual's disease course may vary considerably. --- CD4+ T cell count (cells per µL) --- HIV RNA copies per mL of plasma
The clinical course of infection
Infection with HIV-1 is associated with a progressive decrease of the CD4+ T cell count and an increase in viral load. The stage of infection can be determined by measuring the patient's CD4+ T cell count, and the level of HIV in the blood.
The initial infection with HIV generally occurs after transfer of body fluids from an infected person to an uninfected one. The first stage of infection, the primary, or acute infection, is a period of rapid viral replication that immediately follows the individual's exposure to HIV leading to an abundance of virus in the peripheral blood with levels of HIV commonly approaching several million viruses per mL. This response is accompanied by a marked drop in the numbers of circulating CD4+ T cells. This acute viremia is associated in virtually all patients with the activation of CD8+ T cells, which kill HIV-infected cells, and subsequently with antibody production, or seroconversion. The CD8+ T cell response is thought to be important in controlling virus levels, which peak and then decline, as the CD4+ T cell counts rebound to around 800 cells per mL (the normal value is 1200 cells per mL ). A good CD8+ T cell response has been linked to slower disease progression and a better prognosis, though it does not eliminate the virus. During this period most individuals (80 to 90%) develop an influenza-like illness with symptoms of fever, malaise, lymphadenopathy, pharyngitis, headache, myalgia, and sometimes a rash. Because of the nonspecific nature of these illnesses, it is often not recognized as a sign of HIV infection. Even if patients go to their doctors or a hospital, they will often be misdiagnosed as having one of the more common infectious diseases with the same symptoms. Consequently, these primary symptoms are not used to diagnose HIV infection as they do not develop in all cases and because many are caused by other more common diseases. However, recognizing the syndrome can be important because the patient is much more infectious during this period.
A strong immune defense reduces the number of viral particles in the blood stream, marking the start of the infection's clinical latency stage. Clinical latency can vary between two weeks and 20 years. During this early phase of infection, HIV is active within lymphoid organs, where large amounts of virus become trapped in the follicular dendritic cells (FDC) network. The surrounding tissues that are rich in CD4+ T cells may also become infected, and viral particles accumulate both in infected cells and as free virus. Individuals who are in this phase are still infectious. During this time, CD4+ CD45RO+ T cells carry most of the proviral load.
When CD4+ T cell numbers decline below a critical level, cell-mediated immunity is lost, and infections with a variety of opportunistic microbes appear. The first symptoms often include moderate and unexplained weight loss, recurring respiratory tract infections (such as sinusitis, bronchitis, otitis media, pharyngitis), and oral ulcerations. Common opportunistic infections and tumors, most of which are normally controlled by robust CD4+ T cell-mediated immunity then start to affect the patient. Typically, resistance is lost early on to oral Candida species and to Mycobacterium tuberculosis, which leads to an increased susceptibilty to oral candidiasis (thrush) and tuberculosis. Later, reactivation of latent herpes viruses causes patients to suffer from shingles from Epstein-Barr virus-induced B-cell lymphomas, and from Kaposi's sarcoma, a tumor of endothelial cells that occurs when HIV proteins such as Tat interact with Human Herpesvirus-8. Pneumonia caused by the fungus Pneumocystis jiroveci is common and often fatal. In the final stages of AIDS, infection with cytomegalovirus (another herpes virus) or Mycobacterium avium complex is more prominent. Not all patients with AIDS get all these infections or tumors, and there are other tumors and infections that are less prominent but still significant.
HIV test
Many people are unaware that they are infected with HIV. For example, less than 1% of the sexually active urban population in Africa have been tested and this proportion is even lower in rural populations. Furthermore, only 0.5% of pregnant women attending urban health facilities are counselled, tested or receive their test results. Again, this proportion is even lower in rural health facilities. Since donors may therefore be unaware of their infection, donor blood and blood products used in medicine and medical research are routinely screened for HIV.
HIV-1 testing consists of initial screening with an enzyme-linked immunosorbent assay (ELISA) to detect antibodies to HIV-1. Specimens with a nonreactive result from the initial ELISA are considered HIV-negative unless new exposure to an infected partner or partner of unknown HIV status has occurred. Specimens with a reactive ELISA result are retested in duplicate. If the result of either duplicate test is reactive, the specimen is reported as repeatedly reactive and undergoes confirmatory testing with a more specific supplemental test (e.g., Western blot or, less commonly, an immunofluorescence assay (IFA)). Only specimens that are repeatedly reactive by ELISA and positive by IFA or reactive by Western blot are considered HIV-positive and indicative of HIV infection. Specimens that are repeatedly ELISA-reactive occasionally provide an indeterminate Western blot result, which may be either an incomplete antibody response to HIV in an infected person, or nonspecific reactions in an uninfected person. Although IFA can be used confirm infection in these ambiguous cases, this assay is not widely used. Generally, a second specimen should be collected >1 month later and retested for persons with indeterminate Western blot results. Although much less commonly available, nucleic acid testing (e.g., viral RNA or proviral DNA amplification method) can also help diagnosis in certain situations. In addition, a few tested specimens might provide inconclusive results because of a low quantity specimen. In these situations, a second specimen is collected and tested for HIV infection.
The chemical structure of Abacavir
Treatment
There is currently no vaccine or cure for HIV or AIDS. The only known method of prevention is avoiding exposure to the virus. However, an antiretroviral treatment, known as post-exposure prophylaxis is believed to reduce the risk of infection if begun directly after exposure. Current treatment for HIV infection consists of highly active antiretroviral therapy, or HAART. This has been highly beneficial to many HIV-infected individuals since its introduction in 1996, when the protease inhibitor-based HAART initially became available. Current HAART options are combinations (or "cocktails") consisting of at least three drugs belonging to at least two types, or "classes," of anti-retroviral agents. Typically, these classes are two nucleoside analogue reverse transcriptase inhibitors (NARTIs or NRTIs) plus either a protease inhibitor or a non-nucleoside reverse transcriptase inhibitor (NNRTI). Because AIDS progression in children is more rapid and less predictable than in adults, particularly in young infants, more aggressive treatment is recommended for children than adults. In developed countries where HAART is available, doctors assess their patients thoroughly: measuring the viral load, how fast CD4 declines, and patient readiness. They then decide when to recommend starting treatment.
HAART allows the stabilisation of the patient’s symptoms and viremia, but it neither cures the patient, nor alleviates the symptoms, and high levels of HIV-1, often HAART resistant, return once treatment is stopped. Moreover, it would take more than a lifetime for HIV infection to be cleared using HAART. Despite this, many HIV-infected individuals have experienced remarkable improvements in their general health and quality of life, which has led to a large reduction in HIV-associated morbidity and mortality in the developed world. A computer based study in 2006 projected that following the 2004 United States treatment guidelines gave an average life expectancy of an HIV infected individual to be 32.1 years from the time of infection if treatment was started when the CD4 count was 350/µL. This study was limited as it did not take into account possible future treatments and the projection has not been confirmed within a clinical cohort setting. In the absence of HAART, progression from HIV infection to AIDS has been observed to occur at a median of between nine to ten years and the median survival time after developing AIDS is only 9.2 months. However, HAART sometimes achieves far less than optimal results, in some circumstances being effective in less than fifty percent of patients. This is due to a variety of reasons such as medication intolerance/side effects, prior ineffective antiretroviral therapy and infection with a drug-resistant strain of HIV. However, non-adherence and non-persistence with antiretroviral therapy is the major reason most individuals fail to benefit from HAART.
The reasons for non-adherence and non-persistence with HAART are varied and overlapping. Major psychosocial issues, such as poor access to medical care, inadequate social supports, psychiatric disease and drug abuse contribute to non-adherence. The complexity of these HAART regimens, whether due to pill number, dosing frequency, meal restrictions or other issues along with side effects that create intentional non-adherence also contribute to this problem. The side effects include lipodystrophy, dyslipidaemia, insulin resistance, an increase in cardiovascular risks and birth defects.
Anti-retroviral drugs are expensive, and the majority of the world's infected individuals do not have access to medications and treatments for HIV and AIDS. Research to improve current treatments includes decreasing side effects of current drugs, further simplifying drug regimens to improve adherence, and determining the best sequence of regimens to manage drug resistance. Unfortunately, only a vaccine is thought to be able to halt the pandemic. This is because a vaccine would cost less, thus being affordable for developing countries, and would not require daily treatment. However, after over 20 years of research, HIV-1 remains a difficult target for a vaccine.
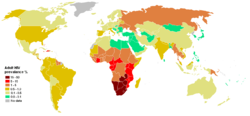
Prevalence of HIV among adults per country at the end of 2005 ██ 15–50% ██ 5–15% ██ 1–5% ██ 0.5–1.0% ██ 0.1–0.5% ██ <0.1%
Epidemiology
UNAIDS and the WHO estimate that AIDS has killed more than 25 million people since it was first recognized in 1981, making it one of the most destructive pandemics in recorded history. Despite recent, improved access to antiretroviral treatment and care in many regions of the world, the AIDS pandemic claimed an estimated 2.8 million (between 2.4 and 3.3 million) lives in 2005 of which more than half a million (570,000) were children.
Globally, between 33.4 and 46 million people currently live with HIV. In 2005, between 3.4 and 6.2 million people were newly infected and between 2.4 and 3.3 million people with AIDS died, an increase from 2004 and the highest number since 1981.
Sub-Saharan Africa remains by far the worst-affected region, with an estimated 21.6 to 27.4 million people currently living with HIV. Two million [1.5–3.0 million] of them are children younger than 15 years of age. More than 64% of all people living with HIV are in sub-Saharan Africa, as are more than three quarters of all women living with HIV. In 2005, there were 12.0 million [10.6–13.6 million] AIDS orphans living in sub-Saharan Africa 2005. South & South East Asia are second-worst affected with 15% of the total. AIDS accounts for the deaths of 500,000 children in this region. Two-thirds of HIV/AIDS infections in Asia occur in India, with an estimated 5.7 million infections (estimated 3.4–9.4 million) (0.9% of population), surpassing South Africa's estimated 5.5 million (4.9–6.1 million) (11.9% of population) infections, making India the country with the highest number of HIV infections in the world. In the 35 African nations with the highest prevalence, average life expectancy is 48.3 years—6.5 years less than it would be without the disease.
The latest evaluation report of the World Bank's Operations Evaluation Department assesses the development effectiveness of the World Bank's country-level HIV/AIDS assistance defined as policy dialogue, analytic work, and lending with the explicit objective of reducing the scope or impact of the AIDS epidemic. This is the first comprehensive evaluation of the World Bank's HIV/AIDS support to countries, from the beginning of the epidemic through mid-2004. Because the Bank aims to assist in implementation of national government programmes, their experience provides important insights on how national AIDS programmes can be made more effective.
The development of HAART as effective therapy for HIV infection and AIDS has substantially reduced the death rate from this disease in those areas where these drugs are widely available. This has created the misperception that the disease has gone away. In fact, as the life expectancy of persons with AIDS has increased in countries where HAART is widely used, the number of persons living with AIDS has increased substantially. In the United States, the number of persons with AIDS increased from about 35,000 in 1988 to over 220,000 in 1996.
In Africa, the number of MTCT and the prevalence of AIDS is beginning to reverse decades of steady progress in child survival. Countries such as Uganda are attempting to curb the MTCT epidemic by offering VCT (voluntary counselling and testing), PMTCT (prevention of mother-to-child transmission) and ANC (ante-natal care) services, which include the distribution of antiretroviral therapy.
Alternative hypotheses
A small minority of scientists and activists question the connection between HIV and AIDS, the existence of HIV itself, or the validity of current testing methods. These claims are considered unsupported by most of the scientific community, who accuse the dissenters of selectively ignoring evidence in favor of HIV's role in AIDS and irresponsibly posing a threat to public health by discouraging HIV testing and proven treatments.
AIDS dissidents assert that the current mainstream approach to AIDS, based on HIV causation, has resulted in inaccurate diagnoses, psychological terror, toxic treatments, and a squandering of public funds. Dissident views have been widely rejected, and are considered pseudoscience by the mainstream scientific community.
Notes and references
HUMANS:
A taste for adventure capitalists
Solar Cola - the healthier cola alternative
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
This
website
is Copyright © 1999 & 2007 NJK.
The bird |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
AUTOMOTIVE | BLUEBIRD | ELECTRIC CARS | ELECTRIC CYCLES | SOLAR CARS |